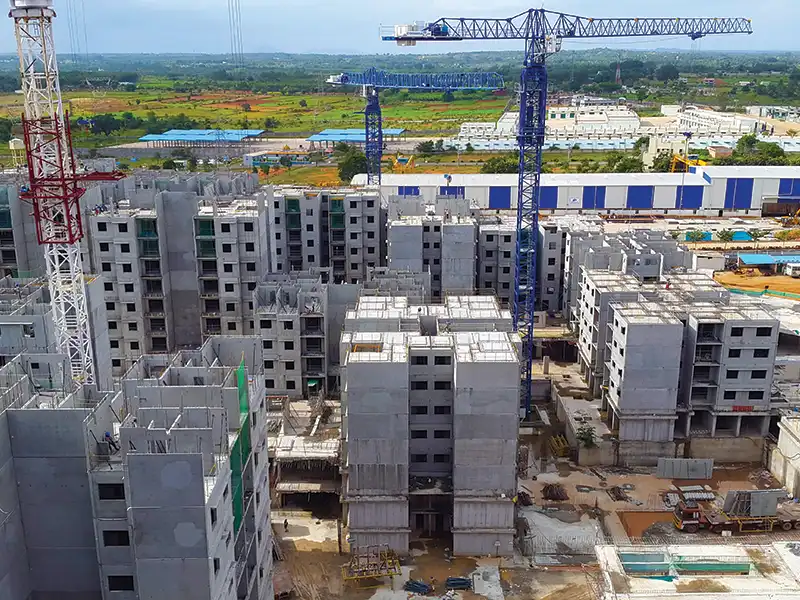
Construction Dust Causes, Effects and Remedies

Construction dust can seriously damage the health of construction workers and if exposed for longer times can eventually even kill them. About 22,000 to 52,000 persons per year are dying due to inhaling polluted air in USA alone – most of whom are construction workers. In Great Britain, over 500 construction workers are believed to die every year from lung cancer. America and Europe have enacted rules to mitigate the effects of dust.
In India, though there are several regulations like the Factories Act, 1948, Mines Act, 1952, Metalliferous Mines regulation, 1961, and Building and Other Construction Workers (Regulation of Employment and Conditions of Service) Act, 1996 and Rules, they specify much higher limits of particulate matter and silica dust which are harmful to construction workers. Moreover, these limits are rarely imposed. The rules directed towards construction water disposal, plastic bags, or smoke emitted from chimneys of cement plants are good, but often present only on paper and rarely implemented.
Published on:
03 April 2019
Published in: NBM&CW April 2019
Share:
We Value Your Comment